Clinical Evaluation of the Foot for Peripheral Arterial Disease

Blogs
Blogs
Clinical Evaluation of the Foot for Peripheral Arterial Disease

Peripheral arterial disease (PAD) and its more severe variant critical limb ischemia (CLI) can be notoriously difficult to diagnose.
When evaluating a patient for PAD we look for certain clinical findings to detect that the patient has or does not have the disease. There are a variety of statistical terms we use to discuss the validity of these clinical findings such as sensitivity, specificity, negative predictive value, positive predictive value, true/false positive/negative and etc.
Some of the common findings we look for are abnormal pulses, bruits (abnormal sounds from arteries), temperature differences, trophic changes (absent hair, thin dry skin, thickened nails), color changes and capillary refill. Many of these findings, when present, are good predictors of PAD. However, if these findings are not present it does not mean that there is no PAD. In short, the negative predictive value of clinical findings for excluding clinically significant PAD is low.
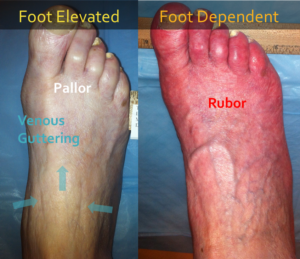
Clinical findings of little value: Berger's Test (Examining the leg after elevation and then in a dependent position. With elevation, the foot turns pale and there can be venous guttering (all the blood has drained out of the veins). When in a dependent position, the foot turns brightly red, called rubor, before returning to a normal pink color. This clinical test, when positive, is a good predictor of a patient have PAD and CLI, but when negative, it does not mean there is not significant PAD or CLI.
Clinical findings of little value: Trophic changes including absence of hair, thickened nails and dry, shiny, scaly skin.

Clinical findings of some value: Pulse palpation. Palpating for pedal pulses is problematic. There are 2 pulses in the foot that to check for - the dorsalis pedis artery (DPA) and the posterior tibial artery (PTA). Pulses are graded on a scale from 0 (absent) to 4 (bounding). There is significant inter-observer disagreement - meaning that 20-40% of the time 2 different examiners do not agree on the grading of the pulse. More significantly, there can be significant blockages in the arteries distal to the area of pulse palpation. In particular, there can be occlusions of the DPA in the mid foot when it is palpable near the ankle. Or the medial or lateral plantar arteries, which are branches from the PTA, maybe blocked causing significant foot ischemia. In about 10% of patients the DPA is congenitally absent. In about 2% of patients, the PTA is congenitally absent. Too often, medical providers palpate a single pulse in the foot and make the incorrect decision that there is adequate blood flow. In reality there are only 2 types of pulses - completely normal or abnormal. Grading pulses is not helpful.
See https://ispri.ng/0YQNr for a typically example of how a the palpation of the PTA lead to delayed revascularization.
This is very concerning. Too many physicians and providers mistakenly think that the absence of these findings means that the patient does not have PAD or CLI. In the worst case scenario, patients with CLI undergo amputation without any proper physiologic testing. All of the clinical findings of PAD and CLI have limited negative predictive value. In other words, the clinical exam is good at saying that a patient has PAD/CLI but it not good at excluding PAD/CLI. Do not make treatment decisions about a patients limb without physiologic testing.